1 Ethical problems in psychiatry- Theories and models of reflection -by zoran.apostolovski19@bathspa.ac.uk
Many ethical issues in medicine are related to very uncommon scientific circumstances and also are an almost day-to-day the obstacle for mental wellness groups. We describe the honest issues that emerged in relation to a substantial difference of opinion between staff member regarding making use of nasogastric clozapine in the therapy of a drastically sick client. We review how conflicting feelings, as well as point of views within groups, obtain honest relevance and also just how the arrangement and also, reflection is necessary for good-quality honest reasoning to happen.

“…the way that we learn from an experience in order to understand and
develop practice”
Psychiatric research study has increased incredibly over current decades to assist in understanding the current patterns and much better restorative choices for illness. On the other hand, there is also a pattern towards greater rates of retraction of published documents in recent years. Principles is needed to maintain and increase the overall quality and morality of research study. Psychiatric research study deals with numerous unique ethical difficulties. Ethical standards are a really essential tool of research study and safeguards participants. The present paper intends to review offered ethical problems and standards relating to psychiatric research study.
Psychiatric research study has numerous important ethical issues which are different from other medical disciplines. These concerns relate to notified approval, privacy, conflict of interest, therapeutic mistaken belief, placebo related, vulnerability, exploitation, operational obstacles, to name a few. The present paper has actually made a number of suggestions to deal with ethical obstacles frequently faced in psychiatric research study.
The ethical guidelines are of utmost requirement for Indian psychiatric research. Particular standards are doing not have pertaining to psychiatric research. The issues and suggestions benefit further conversation and factor to consider.
The term reflection was first identified as
a separate special style of thinking as early as 1933 by Dewey
The primary idea of Dewey became more influential and structured by Schön in 1983


References
Critical Thinking Academy,
2021. Critical Thinking Academy. [Online]
Available at: https://criticalthinkingacademy.net/index.php/ct/benefits-of-critical-thinking
[Accessed 27 May 2021].
Farrell, T. S. C., 2012. Reflecting on Reflective Practice:
(Re)Visiting Dewey and Schon. TESOL International Association, March,
3(1), pp. 7-10. doi:10.1002/tesj.10
Finlay, L., 2008. The Open University. [Online]
Available at: http://oro.open.ac.uk/68945/1/Finlay-%282008%29-Reflecting-on-reflective-practice-PBPL-paper-52.pdf
[Accessed 26 May 2021].
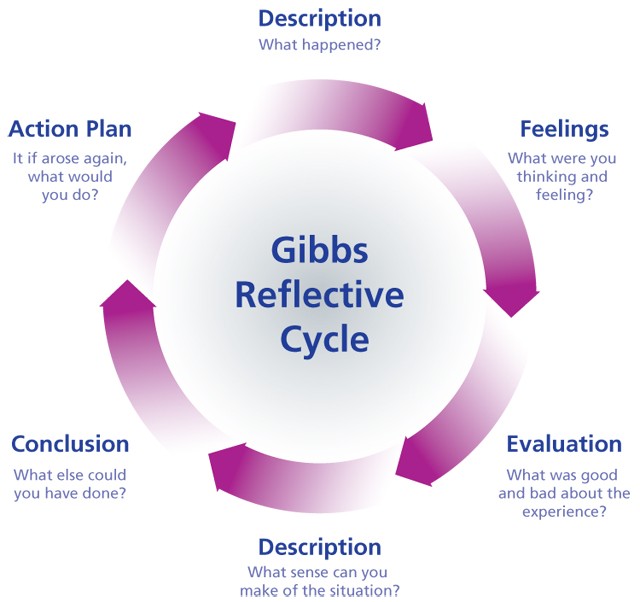
Gibbs, G., 1988. Learning by Doing: A guide to teaching
and learning methods. Oxford: Oxford Brookes University.
Hegarty, B., 2011. Is reflective writing an enigma? Can
preparing evidence for an electronic portfolio develop skills for reflective
practice?. s.l., ResearchGate, pp. 580-593. [Online] Available at: https://www.researchgate.net/publication/267824820_Is_reflective_writing_an_enigma_Can_preparing_evidence_for_an_electronic_portfolio_develop_skills_for_reflective_practice [Accessed 28 May 2021].
Jasper, 2013. ELS. [Online]
Available at: https://www.qmu.ac.uk/media/5533/reflection-2014.pdf
[Accessed 26 May 2021].
Aveyard, H. (2015) (2013) A Beginner's Guide To Critical Thinking And Writing In Health And Social Care (UK Higher Education Humanities & Social Sciences Health & Social Welfare). Paperback.
Fook, J. (2012. 1st Edition. Critical Reflection in Context: Applications in Health and Social Care Routledge
Free Ethical Learning and Development Resource for People and Organisationshttp://www.businessballs.com/reflective-practice.htm
Dresser R (1986). Life, death, and incompetent patients: conceptual infirmities and hidden values in the law. Arizona Law Review, 28, 3: 373-405
Dworkin R (1986). Autonomy and the demented self. Milbank Quarterly 64 (suppl. 2): 4-16
Baldwin C, Hope T, Hughes J, Jacoby R and Ziebland S (2005).Making difficult decisions: the experience of caring for someone with dementia. Alzheimer’s Society
Gastmans C (2013) Dignity-enhancing nursing care: A foundational ethical framework.Nursing Ethics, 2, 42, pp. 142-9
Agich GJ (2003). Dependence and autonomy in old age.Cambridge Univesity Press.